You’ve been diagnosed with Mesothelioma. Now What?
Surgery?
Chemotherapy?
Radiation?
Immunotherapy?
Is Surgery Advisable? Who decides whether it’s “Resectable?”
Most pleural mesotheliomas are potentially operable. The clinical term for that is “resectable.” Many factors influence the resectability of the mesothelioma. Variables include the cell type (epithelial vs sarcomatoid vs biphasic), lymph node involvement, the fitness of the patient, and whether the tumors have spread to other organs, such as the lung itself.
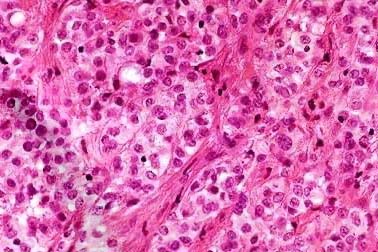
Epithelial cell type
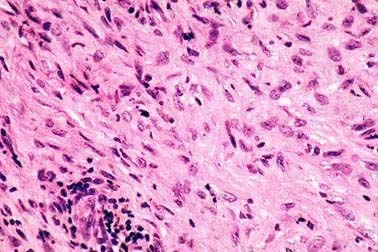
Sarcomatous cell type

Another big variable is this: Who decides? Mesothelioma is a rare and difficult disease to both diagnose and treat. Few doctors, even surgeons, have the experience to credibly make the call whether the tumor is “resectable.” There’s a debate between thoracic surgeons on whether mesothelioma is resectable. For decades now the only surgery thought to be helpful was a complete removal of the lung inside the tumor, aka, “extra-pleural pneumonectomy” (the EPP).
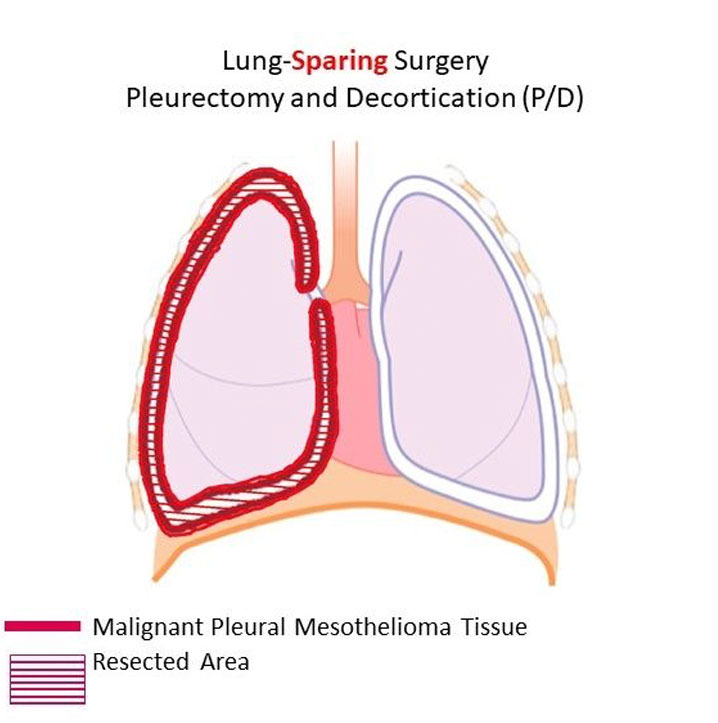
A small but growing group of surgeons, led by Dr. Robert Cameron at UCLA Medical, has shown the best surgery is the “pleurectomy/decortication,” or P/D, a procedure in which the surgeon must meticulously remove the tumor from the ribcage, diaphragm and lung itself. The EPP takes about 2.5 hours. The P/D takes around 10 hours. So, you can see why many surgeons shy away from the P/D.
Nationwide, there are many more oncologists than thoracic surgeons. For decades, most experts have agreed that surgery with radiation offers a greater chance for longer survival than chemotherapy alone (such as Alimta-Cisplatin). Now we’re seeing ads on television touting Opdivo/Yervoy as an immunotherapy option. We applaud the pursuit by drug companies to find meaningful treatments for meso patients. However, there is no data to suggest that Alimta-Cis or Opdivo/Yervoy offer meso patients a better chance of longer survival than any multi-modal approach that includes surgery at its foundation.
It’s well known that surgeons will prefer surgery, and oncologists will prefer chemotherapy or immunotherapy. They prefer what they know. So, should you automatically trust the judgment of an oncologist who has just advised you that your tumor is NOT resectable? That your best option is to hook up to the last cocktail of chemotherapy or immunotherapy drugs that are in fashion?
We don’t think so. Would you trust a bone doctor to tell you whether your heart disease needs surgery? What treatment course to pursue is both the first and most important decision you will make. You should make sure you get an opinion on the resectability of your meso tumor by a thoracic surgery with years of experience in actually removing meso tumors from the human chest.

The purpose of surgery is to remove all visible tumors, thereby relieving pressure which the growing tumor places on the internal organs and preventing the tumor from spreading to other parts of the body. Removing tumor bulk can also offer pain relief, as a growing tumor will compress against the lung, ribcage, heart and nerves.
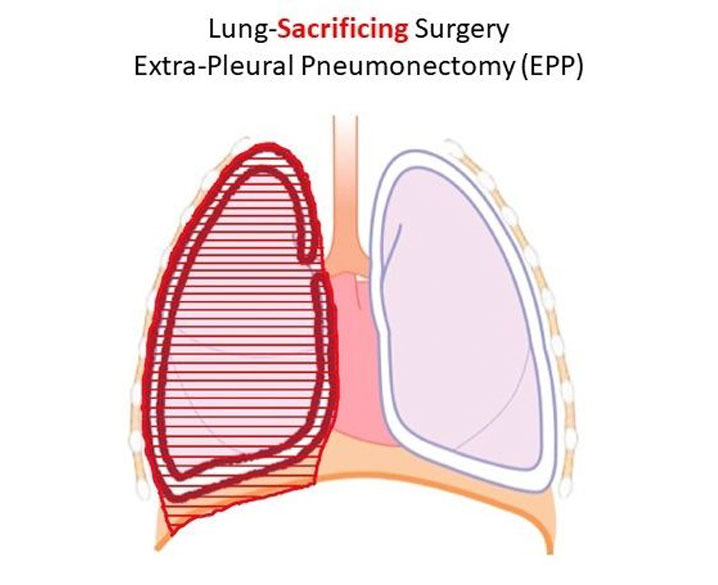
As mentioned above, there are two surgical procedures which are used for treating mesothelioma: the Extrapleural Pneumonectomy (EPP) and the Pleurectomy /Decortication (P/D).
Surgery is the foundation of a successful multi-modal treatment plan. See the video above to better understand the typical progression of mesothelioma. The first question to ask: Is the tumor operable? Only an experienced thoracic surgeon can credibly answer that questions.
The EPP, is a radical procedure where the surgeon removes the lung on the side of the mesothelioma cancer along with the pleura lining the chest wall on that side, the diaphragm (thin breathing muscle) on that side, maybe the pericardium (the sac around the heart), and any nearby lymph nodes. The diaphragm and the pericardium are then rebuilt with man-made materials.
Because of the radical nature of this procedure, and the fact that the patient will be left post-operatively with only one lung, it can only be performed on patients who meet certain criteria such as good cardiac and pulmonary functioning.
The P/D, is a less radical procedure in which all of the pleura lining the chest wall (on the side with the mesothelioma cancer) is removed, along with the pleura coating the lung on that same side. The pleura coating the mediastinum and the diaphragm is also removed. The lung and diaphragm muscle are not removed.
The type of surgery also depends on the hospital and surgeon’s experience along with the details of each patient’s cancer and overall health.